

Last Updated on 2 months ago
Are you interested in reconstructing your breasts with your tissue using the blood vessels and tissue from your abdomen? A DIEP Flap might be an option for you if you haven’t had a prior tummy tuck. DIEP (Deep Inferior Epigastric Perforator) is considered the gold standard of reconstruction and is the first preferred donor site. If you had a prior tummy tuck or are very thin, it’s worth looking into secondary flap options that don’t take muscle such as SGAP, TDAP/TAP, PAP Flaps as well as stacked flaps, and hybrid flaps (implant plus flap).
Questions I Wished I had asked in my First Plastic Consult for DIEP Flap Breast Reconstruction
I first consulted with a local plastic surgeon in Oregon for a DIEP flap, then got many more opinions remotely. I learned so much in the process and compiled this list to help you ask questions when interviewing your team along with answers I received at my first plastic reconstruction appointment versus my final experience. Remember that you are your best advocate and it’s 100% worth getting multiple opinions and comparing.
*Pro tip, ask these questions to multiple plastic surgeons in remote or in-person consults and compare answers to make an informed decision about your team. Consider storing the answers of each plastic surgeon in a spreadsheet to compare when choosing your team. Consider setting up multiple remote consults at the same time so you can compare answers from multiple facilities and surgeons around the same time to make an informed decision.
- How many DIEP Flaps do you do per week/month? My local surgeon performed one DIEP flap per month, but I ended up traveling for surgery where my surgeon did 4 DIEP Flaps per week.
- What is your success rate? My local surgeon wouldn’t quote me his success rate, only the national average. Ideally, you are looking for a 99% success rate for your flap to take. Note you do have options if your DIEP flap fails.
- How long (on average) is surgery? I was originally quoted 14-15 hours for a double mastectomy with an immediate DIEP flap (DIEP done at the same time as mastectomy) locally. Where I ended up going, my double mastectomy and DIEP flap was 6.5 hours.
- Do you work with a co-surgeon that is also a microsurgeon? I had multiple people in the operating room, which included an oncologic breast surgeon who performed the mastectomy, a plastic surgeon (who was a microsurgeon), a co-surgeon (also a microsurgeon who assisted), and a PA.
- What is my risk of bulge? My local surgeon quoted me over a 20% chance risk of a permanent bulge. Where I had surgery, my risk was quoted under 1%.
- Do you typically use mesh or would you take muscle due to the anatomy of my blood vessels? If a surgeon says yes to this, please get another opinion. Many times mesh is used to help prevent hernia when muscle is taken. Many DIEP flap surgeons are taking some muscle to harvest the blood vessels. Sometimes there is a time and place for mesh such as if a patient has a prior fascia injury and needs to strengthen the abdominal wall, that said, if a surgeon is regularly using mesh in their DIEP flaps, know there are other options that don’t include mesh. If a surgeon says that there are times they would take muscle due to your blood vessel anatomy, then know there are other options such as Apex and SIEA, see next question.
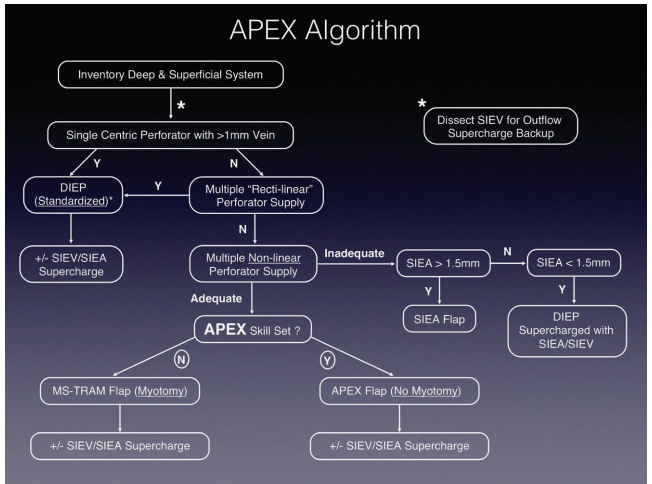
- Are you skilled in the APEX flap technique or SIEA if needed? APEX is a highly specialized skillset that can be used when a patient has complex blood vessel anatomy in the abdomen that prevents any muscle from being taken. There are surgeons who are skilled in this across the US, but they are few and far between. Sometimes, Apex can’t be performed due to inadequate blood supply. SIEA (Superficial Inferior Epigastric Artery) is an alternative way to harvest the blood vessels without compromising the muscle. Important to get multiple opinions as each case is unique.
- I had multiple non-linear perforators (shown in a CTA scan that my local plastic surgeon ordered) and every every surgeon I spoke to wanted to take some muscle, convert to MS-Tram (all tram flaps take muscle), and use mesh. Apex flap is a highly specialized technique where if a patient has multiple non-linear perforators and adequate blood flow, the surgeon will cut the blood vessel behind the muscle, bring it around the muscle, reattach it, and then transfer it to the breast, leaving the abdominal rectus muscle in-tact.
- Would a CTA Scan determine my eligibility for a DIEP? If a surgeon says your CTA scan would determine your eligibility, please get another opinion. Ideally, you are looking for a surgeon who uses your CTA scan as a roadmap to help guide the decision-making process. Below is the Center for Restorative Surgery’s Apex Algorithm (shown on page 3 of the journal article).
- Do I have the option for immediate reconstruction? If you don’t have the option to do a mastectomy and DIEP flap at the same time due to surgeon availability, then please get another opinion.
- Do I have enough tissue for DIEP? If your surgeon tells you to go home and gain weight for DIEP, please get another opinion. I was originally told by my local surgeon to go home and eat hamburgers and milkshakes. I did get multiple opinions and found a surgeon that could work with what I had and I personally was able to achieve my goal size. Note if a patient is athletic with little fat, learn about potential options that don’t compromise the muscle such as PAP, SGAP, Stacked Flaps (such as DIEP + PAP, DIEP + GAP, DIEP + TAP/TDAP) or Hybrid flaps (flap plus an implant).
- Do I need to lose weight for DIEP? If a surgeon explains that you need to lose weight for DIEP, it’s still worth getting another opinion. I know multiple women with high BMI who travel for DIEP who did not have to lose weight to get their surgery.
- Is there an option to fix Diastasis Recti (if relevant) in Phase 1 or Phase 2? Diastasis recti can happen after pregnancy, when your abdominal muscles split. This happened to me, and my surgeon fixed my Diastasis recti during my DIEP and double mastectomy. Not all surgeons offer this.
- What is the backup plan if my flap fails? While DIEP flap failures aren’t common, they can happen. If your surgeon only offers an implant as the backup plan (and you want to use your own tissue), know that there are many alternative donor sites available, but your surgeon may not be skilled in them or have a cosurgeon to help with more complex flaps.
- Ask about options for Nipple Sparing Mastectomy (NSM), Areola Sparing Mastectomy, and Nipple Reconstruction. Note that if you have an areola sparing mastectomy (keep the areola but remove the nipple) that it may limit your nipple tattooing options.
- Show me before and after photos of your DIEP flaps (immediate vs delayed, whatever is relevant to your case).
- Is lowering the scar an option in phase 2? Mine was lowered in phase 2 and my incision is easily covered in a bikini.
- What does Phase 2 entail? When does Phase 2 typically happen? You may be wondering what phase 2 is. Typically, the first surgery is about removing the breast tissue (in immediate reconstruction) and harvesting the blood vessels and tissue for the flap to take. Note that not all patients have a revision/phase 2 surgery but many do.
- There is typically a second surgery (aka phase 2) – (mine was three months after my initial DIEP) to address any concerns and help even them out with lipo/fat grafting. My Phase 2 consisted of extending my incision behind me for better contouring, removing dog ears, and moving fat from my love handles and upper flanks to my chest. Everyone’s phase 2 is different and unique to each person.
- When would my DIEP flap take place? If you are quoted a long waiting period, then please get another opinion (get multiple opinions regardless). Note if you have active cancer there are places that save dates for active cancer that will allow for immediate reconstruction (depending on each situation).
- How many nights would I stay in the hospital? I was originally quoted 3-4 days in the ICU plus another few days in the hospital. I ended up staying 2 nights in the hospital in a private room with ICU-type care (my flaps were monitored with dopplers and nurses checked my flaps every hour for the first 24 hours).
- What should I expect for recovery? My local surgeon told me I would feel like I was hit by a bus for 2 months and would be hunched over on a walker for two months. I was able to stand up straight after about a week and never used a walker. Most of my restrictions were lifted at 4 weeks, with the rest of my restrictions lifted at 6 weeks.
- What items do I need to purchase for recovery? Ask if you would need to purchase a binder, surgical bras, etc for recovery. I put together a list of what to bring to the hospital for DIEP and other helpful items for home.
- How long do I need to stay in town (if traveling for surgery)? I flew into New Orleans a few days before surgery, preop was a day before surgery, 2 nights in the hospital, and I flew home a week after surgery. Note that if a flap fails at home that many times local surgeons won’t want to operate but will send the patient back to who did your surgery. While I flew home after a week, there are many practices that want the patient to stay longer such as 2 or 3 weeks (differs by surgeon).Note that if you do go home and there is a problem with the flap that requires surgery, you will likely need to travel back to the surgeon/facility that did your flap, bear that in mind if considering traveling for surgery.
- Are there discounted or free lodging options if traveling for surgery? I stayed at the Hope Lodge for free (funded by the American Cancer Society). A full list of Hope Lodges around the country are the USA is listed here.
- How long is the recovery? What do restrictions entail by week?
- Will I get a new belly button? Explain this process to me
- Where will my incisions be placed? Find out your options for incision placement
- How can I prepare before the surgery?
- Is PT Recommended after surgery?
Surgical Groups to Look Into for DIEP
The below list is a sampling of surgeons/surgical groups across the US.
- NYBRA – offers virtual consults. Location: Great Neck NY
- Dr. Elisabeth Potter – Offers remote consults. Location: Austin, Tx
- Center for Restorative Breast Surgery – offers free remote consults Location: New Orleans, Louisiana
- Dr. Zampell – Offers remote consults. Location: Beverly Hills and Torrance, CA
- UCLA – Location: Los Angeles, CA (doesn’t offer remote consults, but an option for in-person consult)
- PRMA – offers remote consults Location: San Antonio, TX
- Midwest Breast & Aesthetic Surgery – offers remote consults for out-of-state patients. Location: Gahanna, Ohio
- Center for Breast Reconstruction – offers an educational call Location: New York, NY
- Grand Valley Plastic Surgery (Dr. Henderson) – Offers out-of-state remote consults Location: Grand Junction, CO
- Breast Southwest & Aesthetics – offers virtual appointments Locations: Phoenix, AZ, and Chandler, AZ
Sources:
- Myth-Busting the DIEP Flap and an Introduction to the Abdominal Perforator Exchange (APEX) Breast Reconstruction Technique: A Single-Surgeon Retrospective Review
Read the full article here - DIEP Flap Reconstruction
BreastCancer.org – DIEP Flap Overview - Stacked Flap Reconstruction
BreastCancer.org – Stacked DIEP Overview - Autologous breast reconstruction beyond the DIEP: a narrative review of autologous breast reconstruction options beyond the DIEP flap
Review Article



{kind=link}
No comment